There are five main hepatitis viruses, helpfully named A, B, C, D and E. The hepatitis D virus (HDV)—sometimes known as hepatitis delta—is relatively little-known because it can only live alongside the hepatitis B virus (HBV). This means it needs to be acquired at the same time as hepatitis B, or else someone already living with hepatitis B can be infected with it later on. Because of this HDV is known as a satellite virus.
Hepatitis D is the smallest known virus which can infect humans. Its tiny size means it does not contain all the organic machinery it would need to survive on its own. This is why hepatitis D can only survive in the bodies of those also living with hepatitis B—hepatitis D virus particles are actually defective, and have to make use of hepatitis B’s envelope proteins (part of the “skin” that surrounds each virus particle) in order to reproduce themselves and thrive.
It is estimated that, worldwide, approximately 5 per cent of people living with hepatitis B also have hepatitis D—this is around 12 million people. Exact figures are hard to determine, though, due to very low testing rates. HDV coinfection is most common in China, Russia, Africa, the Middle East, parts of Eastern Europe and the Amazonian river basin in South America.
Transmission
The hepatitis D virus is transmitted by infected blood and body fluids. This can happen from direct exposure to blood, through sharing unsterile injecting drug or body piercing equipment, and through unprotected sex. You can protect yourself from both HBV and HDV by:
- vaccinating against hepatitis B
- practicing safer sex (using a condom)
- not sharing injecting equipment, including tourniquets, spoons and filters (use new and sterile injecting equipment for each injection)
- avoiding tattooing, piercing, dental and cosmetic procedures where equipment is not sterilised
- ensuring all equipment is sterilised and no blood to bloodstream contact occurs when undergoing cultural rituals where blood is involved
- following the Blood Rule in sport
- not sharing toothbrushes, razors, needles, syringes, personal hygiene items and grooming aids or any object that may come into contact with blood or body fluids
- covering all cuts and open sores with a plaster or bandage.
- following standard precautions when handling blood spills
Worldwide, populations that are more likely to have both HBV and HDV include indigenous populations, recipients of haemodialysis, and people who inject drugs.
Coinfection & Superinfection
If you acquire both HBV and HDV at the same time, this is called coinfection. If you are infected with HDV after already having hepatitis B, this is called superinfection. Both coinfection and superinfection of hepatitis B with hepatitis D can lead to more severe health complications than HBV infection alone.
Coinfection generally resolves spontaneously after about 6 months, but it can also sometimes lead to a life-threatening or fatal liver failure. Superinfection is the more common form, and leads to more severe liver disease than a chronic hepatitis B infection alone. HDV has also recently been classified as causing cancer, just like hepatitis B and C. In this sense, hepatitis D is the most severe form of viral hepatitis, carrying with it a 70–80 per cent risk of cirrhosis in five to ten years, and liver cancer within ten years.
Symptoms
People with hepatitis D can have more severe symptoms than those who are infected with HBV alone. Symptoms usually appear 3–7 weeks after infection with HDV. They can include:
- Dark urine or clay-colored stools
- Feeling tired
- Fever
- Joint pain
- Loss of appetite
- Nausea, stomach pain, throwing up
- Yellow skin or eyes (jaundice)
Coinfection symptoms vs. superinfection symptoms
The symptoms of coinfection can be different than symptoms of superinfection. People with coinfection can have distinct sets of symptoms during two separate time periods. This is because hepatitis B symptoms can occur at a different time than those of hepatitis D. People with superinfection usually experience rapid and severe symptoms.
Up to 90 per cent of superinfected individuals will develop chronic hepatitis D, and of these around 70 per cent will develop cirrhosis. To compare, around 15 to 30 per cent of those infected with hepatitis B alone develop cirrhosis. The two viruses in combination are the most lethal of all hepatitis infections, with a fatality rate of around 20 per cent.
Genotypes
There are at least eight different strains of HDV, known as genotypes, each with a distinct way in which the disease progresses. Of the more common strains, genotypes 1 and 3 are more severe, and genotype 2 is milder.
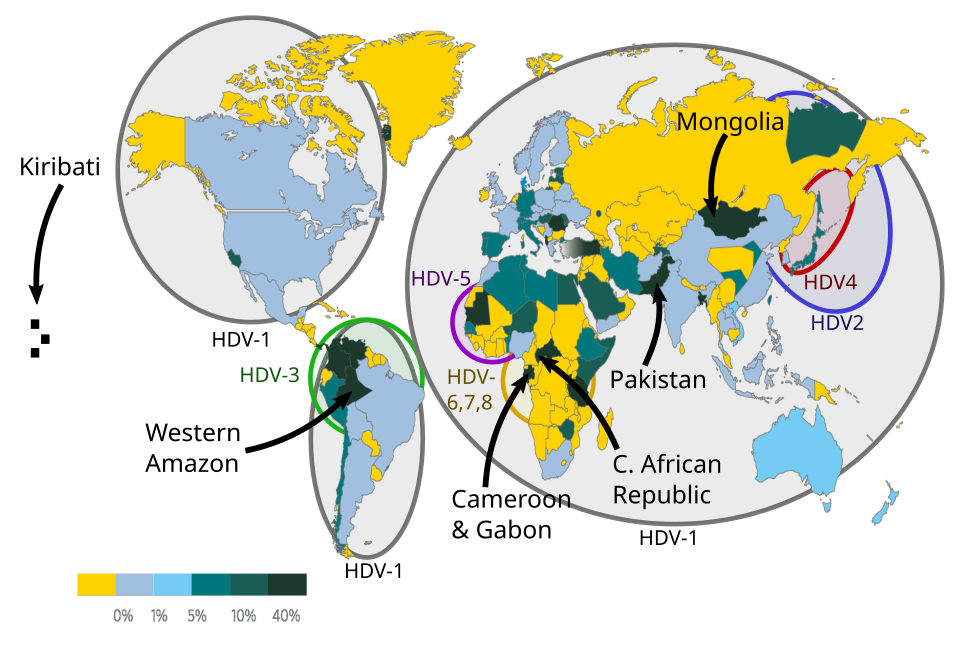
(Image CC via Wikimedia)
Although most people living with HDV have been infected with only a single genotype, multiple exposures to the virus can lead to infections with multiple genotypes, and a more severe reaction to the virus.
Vaccination
Because HDV requires HBV to survive, you can protect yourself by getting vaccinated for hepatitis B. In South Australia, all babies are given this vaccine as part of the National Immunisation Program. Many older people in SA can also receive free hepatitis B vaccination through the state’s High Risk Hepatitis B Immunisation Program.
Testing & Treatment
A targeted treatment, bulevirtide, has been approved by the Therapeutic Goods Administration for use in Australia. It has a much higher efficacy and is more well tolerated than the current treatment options. Buleviritide works by blocking the hepatitis D virus’s access to regenerated liver cells, letting the immune system eliminate the infected cells. This can result in prevention of viral replication, and subsequent reduction in inflammation and associated liver damage. However, Buleviritide is not currently approved for subsidised access through the PBS.
The peak body for health professionals in the field, ASHM, recommends that people living with hepatitis B automatically receive a hepatitis D antibody test. Anyone testing positive for hepatitis D antibodies should then have a hepatitis D PCR test to confirm active infection and inform clinical care. This automated testing process is known as double reflex testing. For those who go on treatment, twice-yearly monitoring via hepatitis D PCR tests is then extremely important.
If you’re living with hepatitis B or D, please talk to your liver nurse or specialist about your options.
Last updated 6 March 2026
More from:
Enjoyed this article? Subscribe to be notified whenever we publish new stories.
Subscribe for Updates