There is a true story about Helen, who for 12 years, lived with hep C without hep C. She lived with the feeling of guilt, isolation and anxiety until she discovered inadvertently that she didn’t have hep C. Her doctor had failed to order the second test required to confirm her hepatitis C status.
On the flip side, another person told of how he’d thought he was safe and protected from hepatitis C because he had hepatitis C antibodies. It was only later—when another healthcare provider ordered the second test—that he found out he in fact had hepatitis C and needed further medical care.
Helen’s story would not have happened had she been tested today. South Australia now has a procedure for automatically carrying out the second test to confirm ongoing infection, should the first test indicate past hepatitis C infection.
Hepatitis C testing is usually in two steps: an antibody test to see if the person had been exposed to the hepatitis C virus, followed by a test that looks for the genetic material of the virus called a RNA or PCR test. This checks if the virus is still present. The RNA test is conducted only if the first test returns a positive result, and until recently, needed to be specifically requested by the healthcare provider, even if the first test showed that the person had been exposed to the hepatitis C virus.
This has resulted in people with chronic hepatitis C not being properly diagnosed. In some cases, doctors did not recall patients for the second test, while in others the patient just didn’t show up and became lost to follow-up.

Reflex it
To address this problem, from June this year, SA Pathology has taken the very logical (and common-sense) decision to automatically carry out that second test, should the first test indicate a need for it. This automatic further testing is known as ‘reflex testing’. South Australia is an early adopter of this approach, which has been recommended for quite a while, by clinicians, pathologists, epidemiologists, researchers, community organisations in the viral hepatitis sector, and people affected by hepatitis C across Australia. It is also a priority action in the National Hepatitis C Strategy.
According to the SA Health webpage, “SA Pathology has commenced reflexive NAT (nucleic acid test) testing on all samples that are HCV antibody-reactive or indeterminate, if specimen volume is sufficient.” This means if samples test positive for hepatitis C antibodies or if the results are not clearly negative, the laboratory will go on to test for hepatitis C RNA in those samples, if there is enough sample left for carrying out that next test. Reflex testing, it says, decreases the burden on medical practitioners and patients and minimises delays between initial testing and treatment commencement.
It will also reduce mis- and missed diagnoses—like the examples discussed earlier.

This move is part of a concerted push to eliminate hepatitis C in South Australia by 2030. Untreated chronic hepatitis C infection is a major cause of liver disease, cancer, and premature death. South Australia could be the first jurisdiction in Australia, and among the first in the world, to eliminate hepatitis C as a public health threat.
Key to this campaign is accurate and efficient diagnosis to find people who have been living with hepatitis C without knowing it, and to find re-infections among those who had been cured but are exposed to ongoing risks. Reflex testing is just another tool to make the process easier and faster for medical practitioners and patients.
The SA Health website provides clear advice and recommendations to medical practitioners on routine and repeat testing, serology requests, notifications, and sample collection, among other useful tips such as identification of high-risk settings and clinical indicators.
What about D?
As we celebrate the introduction of reflex testing for hepatitis C, it’s worth noting that there are experts advocating for reflex testing of another viral hepatitis infection – hepatitis D.
Hepatitis D is a viral infection that occurs only in people living with hepatitis B. It is the most severe form of viral hepatitis, with a 70 per cent risk of cirrhosis in five to ten years, and liver cancer within ten years. People at greatest risk of hepatitis D are those with living with hepatitis B who are also from global regions of high prevalence.
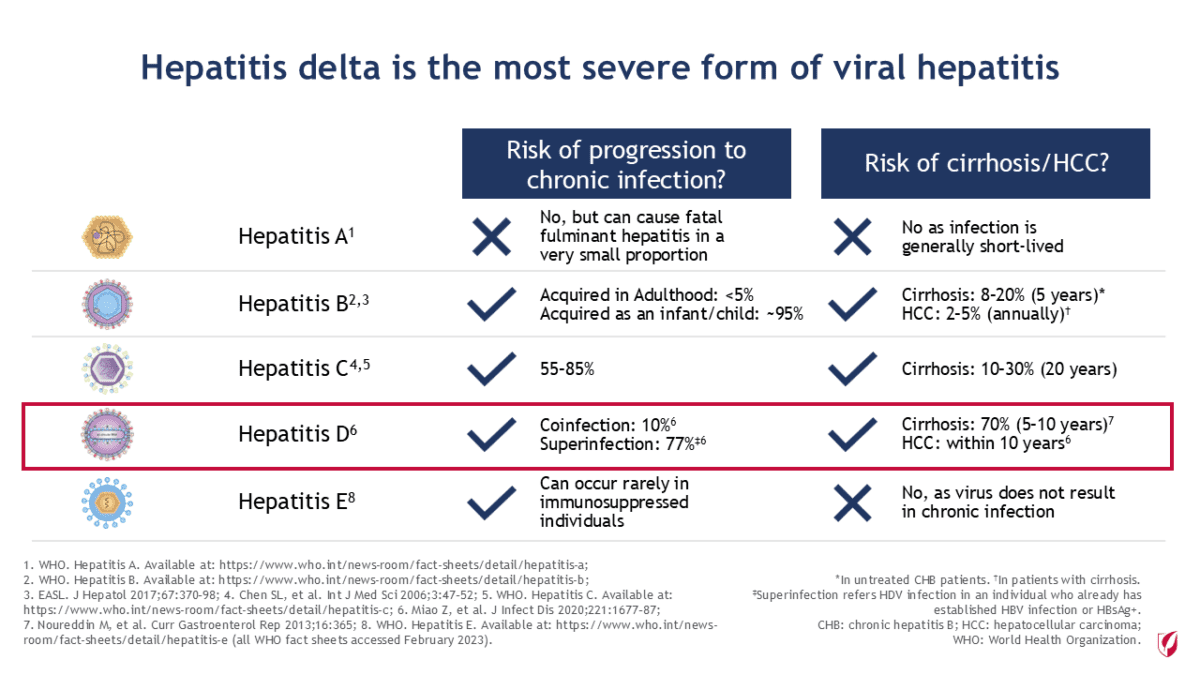
There is not enough data to establish the true prevalence of hepatitis D globally or within Australia but—as can be seen from the numbers—for individuals with hepatitis D, the outcomes can be devastating.
Identification of hepatitis D is a complex process involving many visits, beginning with the identification of chronic hepatitis B infection, followed by testing for hepatitis D antibodies, which is then followed by hepatitis D RNA testing.
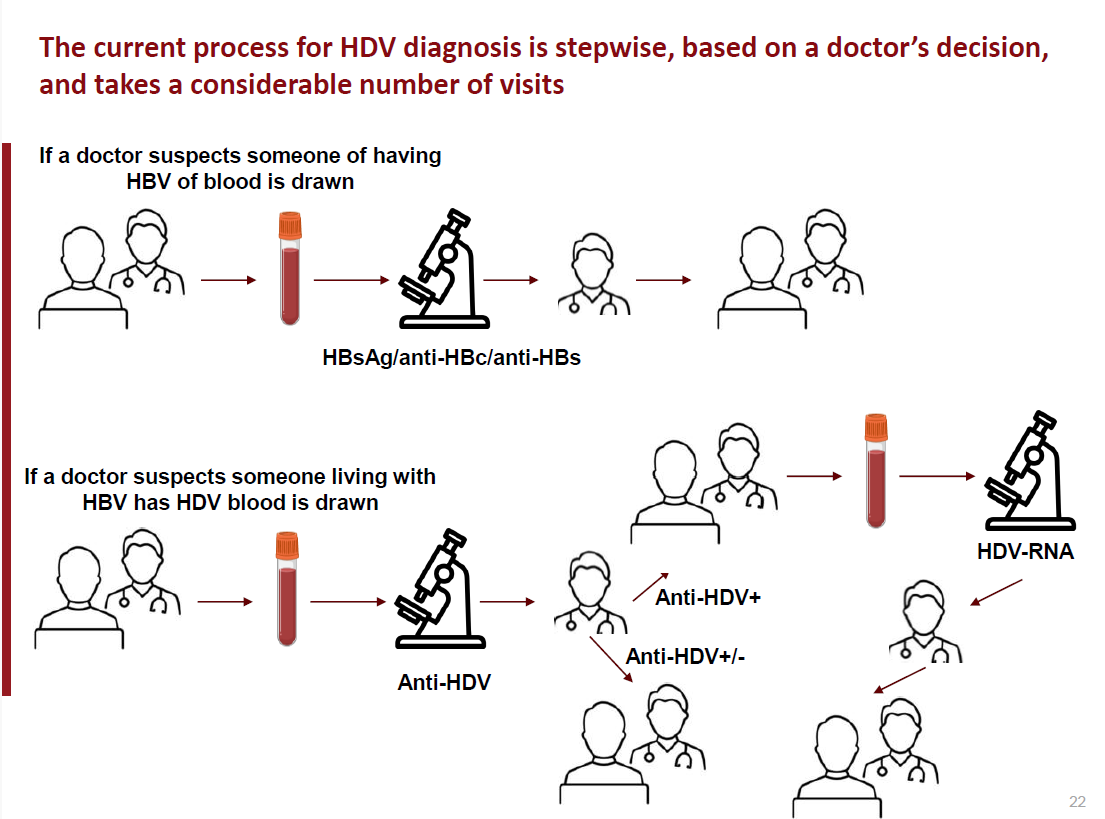
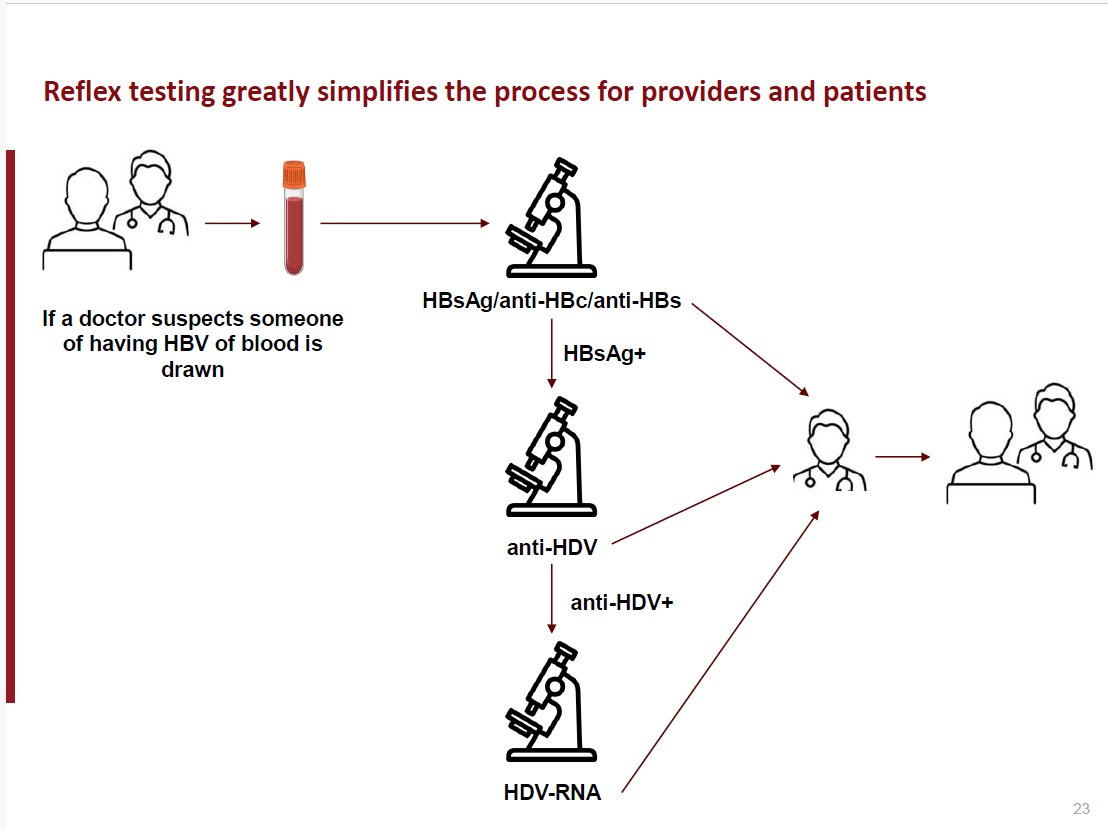
This can be reduced to two visits where a sample tested for hepatitis B is automatically tested for hepatitis D antibodies and hepatitis D RNA when test results indicate the possibility of infection. Reflex testing of hepatitis D for people with chronic hepatitis B will not only identify people who are at real risk of serious disease and death and get them into care, but also provide a better understanding of the prevalence of hepatitis D and the associated burden of care.
With the rising rate of hepatitis B in Australia, it could be time for hepatitis D reflex testing to be put on the agenda.
Source:
- The Case for Hepatitis D (HDV) Reflex Testing, D. Razavi-Shearer, https://www.hepb.org/assets/Uploads/Razavi-Shearer-HDV-Reflex-230914-1-2.pdf
- Increase in routine hepatitis C RNA testing required to achieve elimination, SA Health, https://bit.ly/sahcvreflex
Last updated 28 April 2025
More from:
Enjoyed this article? Subscribe to be notified whenever we publish new stories.
Subscribe for Updates